
During a recent webinar, Rethink Behavioral Health and the Behavioral Health Center of Excellence asked the question: “What does ‘quality’ really mean?” in regards to an Applied Behavior Analysis (ABA) service provider. As you know, ABA providers come in many different forms. But, regardless of the type, each provider presents challenges at both the individual and organizational (i.e. systems) levels.
Let’s look at three types:
In-home providers bring Board Certified Behavior Analysts (BCBAs) and behavioral technicians to the client’s home to deliver services. Factors such as drive time for employees and the geographical area of coverage can quickly become logistical obstacles to deliver effective treatment and supervision if not managed carefully. Moreover, technicians working in homes are often working alone, without other techs in the vicinity to share their experiences.
Center-based providers, on the other hand, forego many of the logistical constraints of in-home providers in that the clients and families come to them. Still, a center presents different challenges not typically seen in an in-home setting. For example, a center often has many clients in relatively close proximity for extended periods, which has safety implications for clients and staff. Additionally, a poorly structured center can have deleterious effects on treatment plans if, for example, clients exhibit disruptive behavior that frequently distracts other clients and staff during their sessions.
Residential providers often combine service-delivery issues from in-home and center-based providers. For example, residential providers typically have a number of homes in a community where clients live in close proximity. Moreover, each house is typically staffed 24 hours a day with behavioral technicians implementing programs, which can further compound the issue. As with in-home providers, however, residential providers often take clients into the community to practice adaptive skills in naturalistic settings, thereby introducing potential logistical issues related to mileage.
Though each provider experiences challenges unique to the settings in which they operate, they all have one thing in common: work processes. Work processes are something about which behavior analysts have talked for a long time, particularly those involved in Behavioral Systems Analysis (BSA). BSA can be thought of as a sister domain to Organizational Behavior Management (OBM) but with a wider focus on the organization as a whole.
From the BSA literature, the concept of metacontingency arises, which refers to a contingent relation between the aggregate product or service of an organization and its consumers. A strong metacontingency ensures the health and survival of the organization. Alternatively, a weak metacontingency requires the organization to adapt if it is to survive.
ABA service providers primarily generate aggregate services, measured in terms of caseloads and how treatment plans are implemented. Primary consumers — the clients, families, and often times insurance companies, have the power to “hire or fire” service providers. They can turn revenue streams on or off based on satisfaction with behavior change outcomes and the methods by which said outcomes are achieved.
However, aggregate services aren’t produced out of thin air, but instead by Interlocking Behavioral Contingencies (IBCs). IBCs occur when an employee’s behavior or behavioral product reliably functions as an antecedent or consequence for another employee’s behavior. Examples include the BCBA who writes programs for his/her techs, supervision given by BCBAs to techs, parent meetings with the BCBA, or staff meetings with managers and employees.
Lastly, IBCs don’t occur in a vacuum but are embedded in a cultural-organizational milieu consisting of a myriad of setting factors both within and outside of the organization that affects work processes. Factors within the organization primarily relate to policies developed, which have effects on IBCs of BCBAs. For example, if policies related to supervision requirements fail to consider the size of the geographical area constituting a BCBA’s case distribution, the productivity of the BCBA may suffer as well as the IBCs connected to the BCBA (e.g. through bottlenecked work processes). Factors outside the organization include insurance policies and activities of state legislatures in which the provider operates. For example, in some states, Medicaid covers ABA services whereas families in other states must seek out services through private insurance. Often times providers operating in Medicaid states acquire large caseloads quickly, as compared to other states.
Below is a graphical depiction of the metacontingency elements:
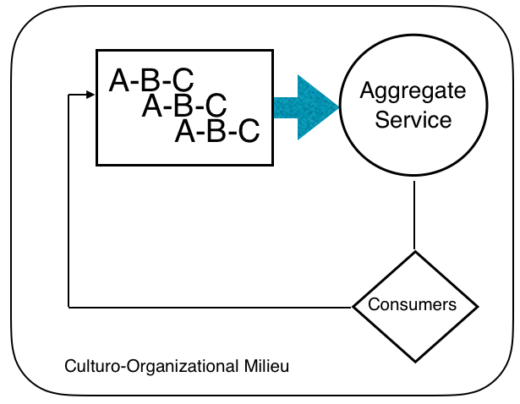
So, when you ask yourself, “What does quality mean?” for your own organization, consider how to precisely define and measure your aggregate service, its fit with the makeup of your consumers, the crucial IBCs that contribute to your service, and the larger policies and laws that influence your IBCs. Process mapping your organization will be much more complex than the simplified graphic above, but the basic elements are there.
About the BHCOE
BHCOE is a trusted source for recognizing exceptional special needs providers that excel in the areas of clinical quality, staff satisfaction and qualifications and consumer satisfaction. Using standardized methods and practices, the organization acts as a third-party to measure and report on existing quality criteria in the behavior analysis community, through interviews with agency clinical leadership, detailed staff qualification review, an anonymous staff satisfaction survey and an anonymous consumer satisfaction survey. BHCOE awards only those service agencies that meet elite standards. For more information, visit http://www.bhcoe.org.
About Rethink Behavioral Health
Rethink Behavioral Health provides the tools every behavioral health provider needs to manage their practice and deliver quality ABA treatment effectively & efficiently. Rethink’s easy to use web-based software streamlines client care with sophisticated yet intuitive tools for both clinicians & administrators. For more information, visit http://www.rethinkbh.com.
REFERENCES
Glenn, S. S. (2004). Individual behavior, culture, and social change. The Behavior Analyst, 27, 133-151.
Glenn, S. S. & Malott, M. E. (2004). Complexity and selection: Implications for organizational change. Behavior and Social Issues, 13, 89-106.
Houmanfar, R. A., Rodrigues, N. J., & Ward, T. A., (2010). Emergence & Metacontingency: Points of Contact and Departure. Behavior and Social Issues, 19, 78-103.






{kind=link}